Par le Docteur Frédéric Braccini
Botulinum toxin is a fantastic tool which, by relaxing the muscles, leads to the temporary disappearance of facial wrinkles. But the best thing is that it can also be used to alter the balances between the agonist and antagonist muscles in the face.
With age, the strength and action of the depressor muscles tends to dominate that of the elevator muscles, leading to a sad-looking appearance and lines that lead downwards from the corner of the mouth. As well as smoothing any wrinkles, it is important to rebalance the facial muscles to enable the face to recover its positive energy.
The upper face
The most important balance is the one between the orbicularis muscle, which lifts the frontalis muscle, and the lowering of the lateral part of the eyebrow by the orbicularis muscle.
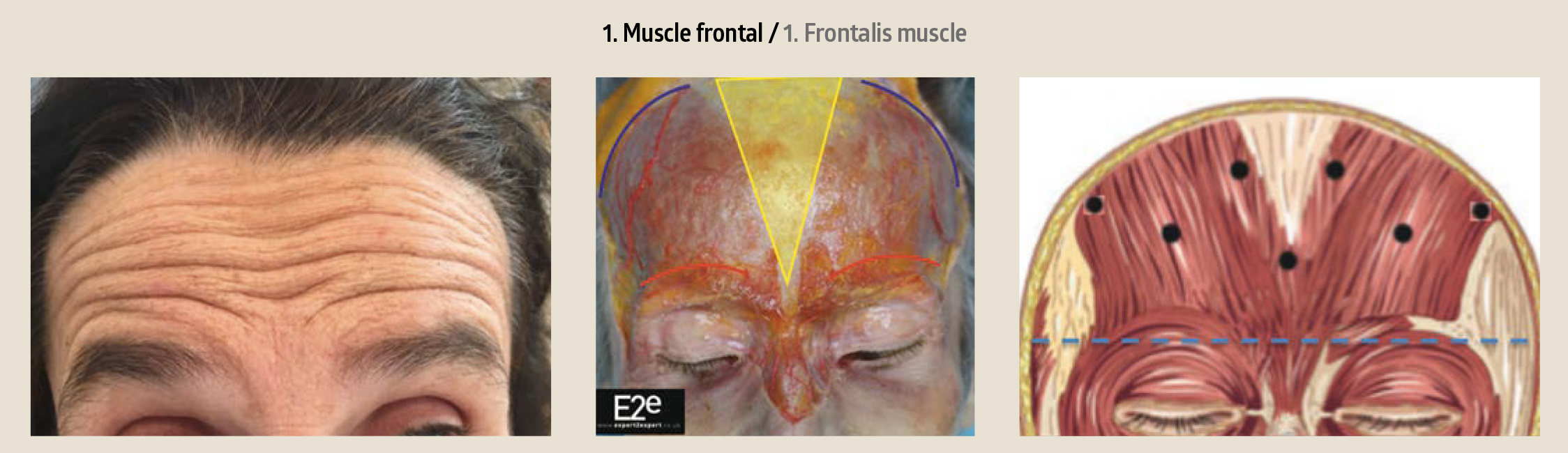
Frontalis muscle
This is the only elevating muscle. Its shape and extension determine the horizontal forehead wrinkles. It allows the tail of the eyebrow to be lifted when its lateral extension is sufficient.
It is the anterior part of the occipital-frontal muscle (digastric muscle: occipital at the back, attached to the occipital bone, and frontalis at the front, joined by the galea aponeurotica). It covers the forehead and glabellar. It is attached to the deep face of the skin, to the inner two-thirds of the eyebrows and the region between the eyebrows. Its inner and mid zones are interlocked with the procerus muscle, in the region between the eyebrows. Its lateral part goes into the deep face of the skin on the inner two-thirds of the eyebrow, where it crosses over the orbital part of the orbicularis muscle and corrugator muscle.
From these cutaneous anchors, its fibres are vertical, on the forehead, before continuing along the galea aponeurotica (occipital-frontal aponeurotic muscle complex).
On the median line, there is most often a V-shaped aponeurotic diastasis between the two muscles. But, sometimes, the two muscles are joined, creating a continuous muscle plane that takes up the whole width of the frontal region.
To the side, its outer edge is located by the temporal bony ridge.
Its contraction creases the forehead and lifts the eyebrow: it is the only elevating muscle of the eyebrow.
We can also consider that, due to its contraction:
• the upper part of the frontalis muscle pulls the hairline down
• the lower part lifts the eyebrow (Figure 1)
Orbicularis oculi muscle
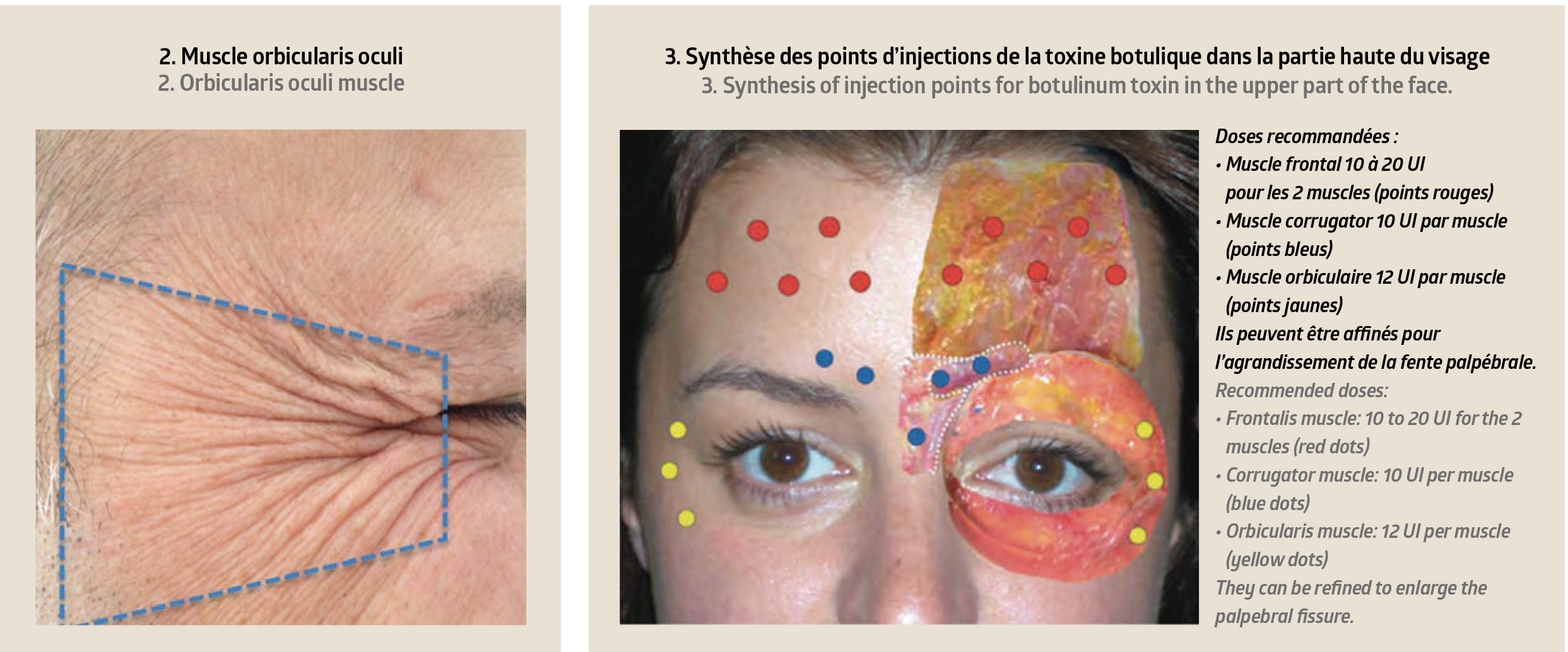
A veritable sphincter for opening and closing the eyelids and pulling down the eyebrow, this muscle has two portions.
Palpebral portion: This covers the tarsus and septum and is comprised of several bundles (pre- and retro-ciliary, pre-tar- sal and pre-septal). It is responsible for the involuntary movements; its reactional hypertonia due to the slight relaxation of its fibres at rest, with age, reduces the opening of the palpebral fissure.
Orbital portion: This forms a large, flat ring that spreads across the whole edge of the eye socket, the anterior part of the temporal fossa, part of the cheek, the frontal apophysis of the jawbone, the facial muscles (corrugator, small zygomatic, elevator of the upper lip). It is responsible for the voluntary movements; it pulls the eyebrows down and creates crows’ feet wrinkles (Figures 2-3-4).
Lower face
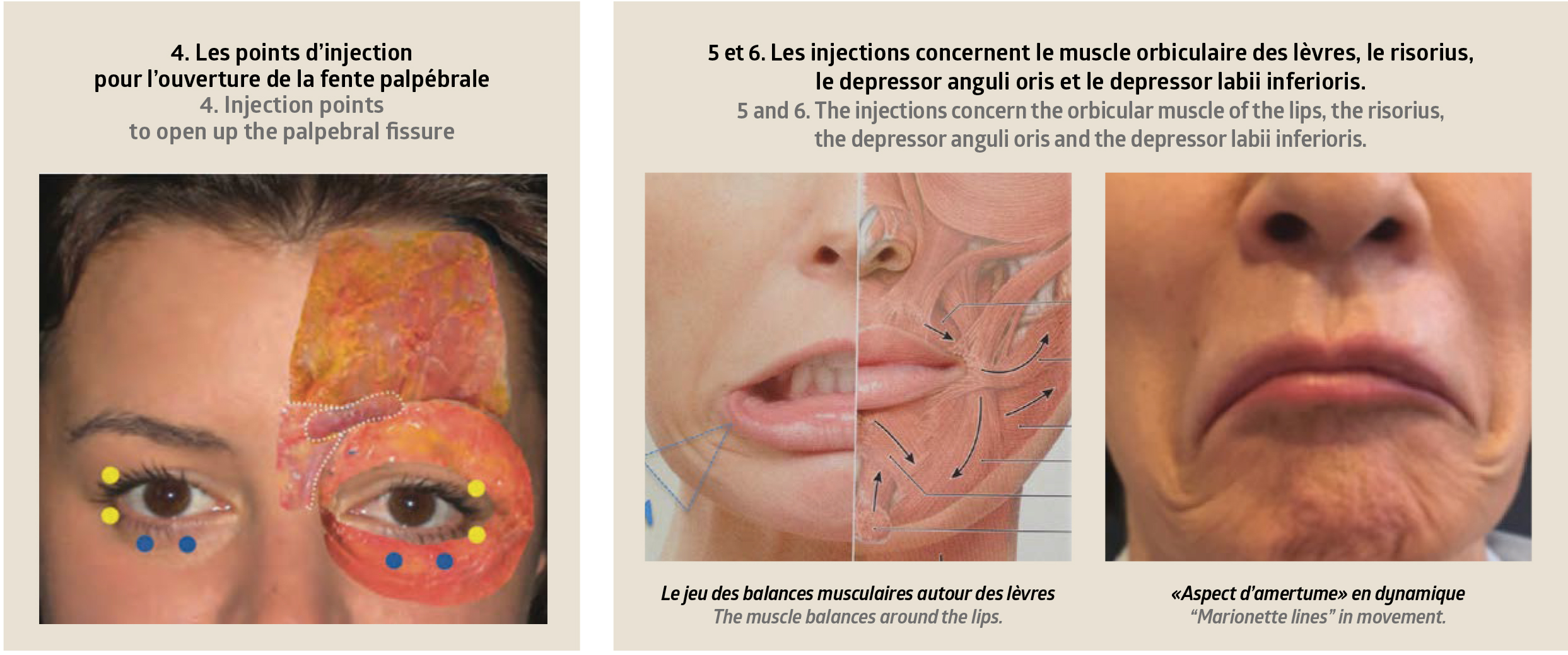
This is the “battle” between the DAO (depressor anguli oris) muscle and the elevator muscles, primarily the zygomatic muscles, which determine the shape and curves at the corners of the mouth. However, a number of muscles are involved to ensure the orofacial movements.
The depressor anguli oris muscle
This is mainly responsible for marionette lines, the face’s major negative expression.
It is a triangular, 3D-shaped muscle with a large base along the jawline and ending at the corner of the mouth. Its starts deep within the tissue, at the bone, and finishes in the su- perficial layers.
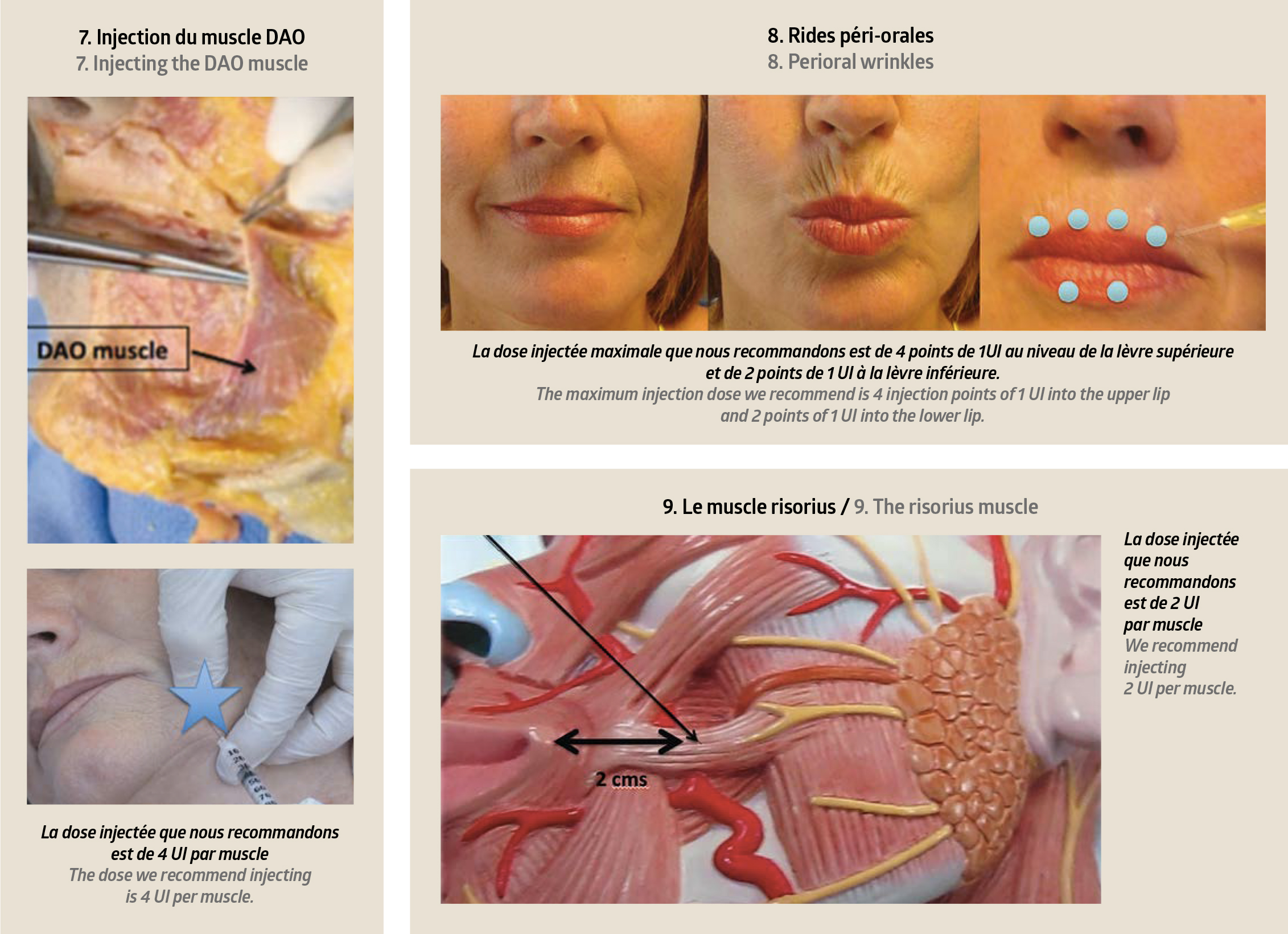
The DAO must be injected at a safe distance from the modiolus, deeply and into where the muscle begins on the jawline, and into the external half of the muscle.
In practice, in order to locate the ideal injection point, we draw a horizontal line one centimetre outside the modiolus, then a vertical line that crosses the edge of the jaw, and it is where these two lines cross that we inject the botulinum toxin. The injection must be perfectly symmetrical, in both its quantity and its position.
The orbicularis oris muscle
This is responsible for “barcode” wrinkles.
It is a concentric, elliptic muscle set around the buccal orifice. Its role as a sphincter makes it an essential muscle for eating, as well as expressions and communication.
We must be very careful when using toxin. This muscle has two distinct parts: a marginal part and a peripheral part. The toxin injections are very superficial, positioned in the wrinkles, on the edge of the vermillion lip, in the median part of each half of the lip, an area which contains motor plates.
It is fundamental not to get closer than a centimetre to the modiolus, because this might lead the product to diffuse to the side. The superior and inferior vertical injection points must be placed along the vertical line.
The efficacy of botulinum toxin on these perioral wrinkles is lesser than in other regions, and the muscles’ motricity generally returns sooner.
The risorius muscle
This is responsible for “dimples”.
It is a small activity muscle whose size varies greatly. It runs from the outside of the parotidean fascia and out towards the skin on the inside of the modiolus.
When injecting, we must stay at least 2cm away from the corner of the mouth (picture 9).
 Par le Docteur Frédéric Braccini
Par le Docteur Frédéric Braccini
ENT, Plastic Surgery of the Face, Nice (France).
Secretary of the French Society of Plastic Surgery of the Face.
Former president and co-founder of the SAMCEP.
Scientific director for the Awards de l’Esthétique Medicale.
More information on braccini.net










