Dr Frédéric Braccini
Rhinoplasty remains one of the most intricate and artistic procedures in aesthetic surgery.
Over the past decade, rhinoplasty has evolved toward more refined, conservative, and less traumatic approaches. The concept of mini‑rhinoplasty offers subtle yet effective correction with limited dissection and faster recovery. Meanwhile, advances in aesthetic medicine — particularly the use of injectable fillers and botulinum toxin — have introduced the era of medical rhinoplasty, offering non‑surgical alternatives for selected patients.

Rhinoplasty is one of the most technically challenging operations in facial plastic surgery due to its three‑dimensional structure and the psychological importance of facial appearance. Each patient represents a unique anatomic and emotional profile, making individualised planning essential. Parallel to surgical evolution, aesthetic medicine has provided additional tools for nasal enhancement. The integration of non‑surgical methods has reshaped the modern philosophy of rhinoplasty. Each adjustment of nasal elements affects adjacent facial volumes; therefore, rhinoplasty must be approached as “facial sculpture,” where balance and proportion guide every movement.
The Mini‑Rhinoplasty Concept
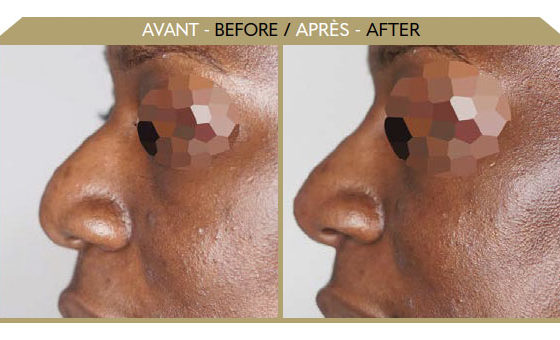
Mini‑rhinoplasty is a limited, conservative surgical technique for small deformities. This approach focuses on subtle contour modification with minimal dissection, performed under local or short general anaesthetic in an outpatient setting.
Surgical Steps
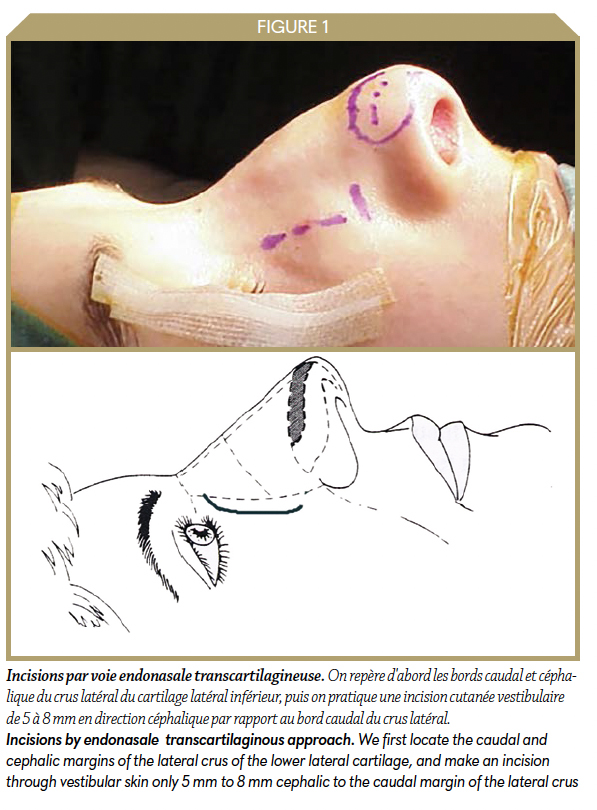
• Incision: Endonasal, transcartilaginous approach.
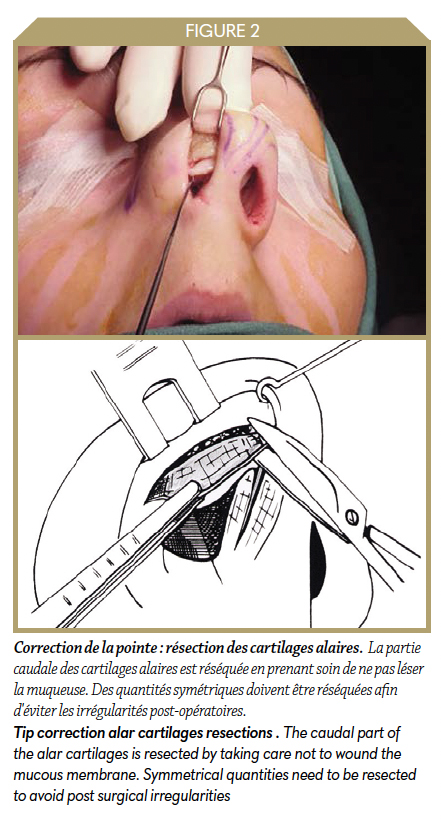
• Cartilage Resection: Controlled removal of the caudal segment of the alar cartilages while preserving mucosa and symmetry.
• Septal Reduction and Hump Removal: Small cartilage resections (< 4 mm), either in two stages (scissors + rasp) or at the same time.
• Osteotomies: Closed lateral osteotomies produce stable repositioning; complete fractures are preferred.
• Final Adjustment: Alar base correction where necessary.
The Rise of Non‑Surgical Rhinoplasty (Medical Rhinoplasty)
Medical rhinoplasty has become one of the signature procedures in modern aesthetic medicine. The combination of fillers with botulinum toxin improves contour, smoothness, and nasal tip dynamics, offering a reversible, low‑risk option. The nasal framework comprises fixed bony‑cartilaginous structures and mobile lower lateral cartilages. Soft‑tissue thickness and skin texture vary, influencing injection depth and diffusion. Vascular anatomy must be respected to avoid ischemic complications. The angular, lateral nasal, and dorsal nasal arteries require cautious technique during injections.
Fillers
Only non‑permanent fillers are recommended. Hyaluronic acid remains the gold standard for nasal contouring. Products with high cross‑linking density provide better structural stability and resistance to migration. We can inject and perform camouflage rhinoplasty before any surgery or to correct after surgery some irregularities (just after the surgery or long time later). Medical rhinoplasty can be placed as “air bags” after surgeries. The filler can also be used to improve functional disorder (nasal valve) essentially after excessive reactions during surgery.
Key techniques:
• Dorsal refinement: slow retrograde linear injection in contact with bone;
• Tip definition: radial injection through one or two entry sites;
• Columellar lift: deep midline injection to open the nasolabial angle.
Botulinum Toxin
Botulinum toxin type A is used mainly for hyperactive nasal muscles. Doses vary per injection site — typically 2.5– 5 IU along the levator labii alaeque nasi, 5 –10 IU at the nasion, and 5–15 IU at the nasal spine. We can also relax all the muscle envelope (transverse muscle, dilator muscles, …). For each point of injection we recommend 2 to 4 IU. Clinical effects last about 3–4 months.
Combined Technique and Outcomes
The dual use of fillers and botulinum toxin enhances nasal shape and expression. Combined protocols yield harmonious, natural results lasting up to 18–24 months for fillers. Our experience with over 3,500 medical rhinoplasties (2008–2026) confirms the safety and satisfaction of this minimally invasive approach.
Future directions will continue to blend surgery and aesthetic medicine, defining rhinoplasty as both a technical and artistic frontier in modern facial aesthetics.
Dr Frédéric Braccini

ENT, Plastic Surgery of the Face, Nice (France). Secretary of the French Society of Plastic Surgery of the Face. Former president and co-founder of the SAMCEP
Infos: www.braccini.net
References
1. Pech A, Cannoni M. La rhinoplastie personnalisée. Springer‑Verlag; Paris, 1993.
2. Anderson JR, Ries WR. Rhinoplasty: Emphasizing the External Approach. New York: Thieme; 1986.
3. Braccini F, Dohan Ehrenfest DM. Combined therapies in aesthetic medicine for facial aging. Rev Laryngol Otol Rhinol (Bord). 2010;131(2):89‑95.
4. Braccini F, Saban Y. Surgical anatomy of the nose. Rev Laryngol Otol Rhinol (Bord). 2006;127(1‑2):9‑13.
5. Saban Y, Braccini F. Rhinoplasties. Monographie du CCA‑Amplifon; 2002.
6. Braccini F, Porta P, Thomassin JM. Mini‑rhinoplasty. Rev Laryngol Otol Rhinol (Bord). 2006;127(1‑2):23‑8.
7. Braccini F, Berros P, Belhaouari L. Botulinum toxin applications in facial wrinkles. Rev Laryngol Otol Rhinol (Bord). 2006;127(1‑2):105‑11.
8. Redaelli A, Braccini F. Medical Rhinoplasty: Basic Principles and Clinical Practice. OEO Edition; Firenze, 2010.
9. Braccini F, Dohan Ehrenfest DM. Medical rhinoplasty using fillers and toxin. Rev Laryngol Otol Rhinol (Bord). 2008;129:233‑8.
10. Dayan SH, Kempiners JJ. Nasal tip ptosis treatment with botulinum toxin. Plast Reconstr Surg. 2005;115(6):1784‑5.
11. Surek CC. Advanced anatomy for injectables. Plast Reconstr Surg. 2021;148(5):983e‑994e.
12. Kim HJ, et al. Vascular complications in filler rhinoplasty: prevention and management. Aesthetic Plast Surg. 2022;46(1):133‑144.
13. Braccini F, et al. Combining surgical and injectable techniques in facial aesthetics: a 2023 perspective. Fac Plast Surg Aesthet Med. 2023;25(4):210‑219.
14. Braccini F, Roman O. The art and science of modern rhinoplasty. Fac Plast Surg Aesthet Med. 2024;26(2):145‑150.