Eduardo Rodríguez Mieles, MD, Dermatologist *

The range of anatomic areas to be injected with HA fillers has gone far beyond the initial and classical indications, like the nasolabial sulcus. Different and somehow challenging indications – not necessarily risky if techniques are adecuate- evolved with time and experience, like the tear through, the temporal hollow, the depression of the middle third of the face, and of course, the nose.
One of the new alternatives in the market is Liquidimplant®, (Nova Cutis Inc., Miami, USA) a monophasic, non animal-based, cross-linked hyaluronic acid (HA) filler gel.
The term “medical rhinoplasty” was first described by Braccini and Ehrenfest in 20081. It consists in the injection of dermal fillers in the external or internal nasal area to modify or improve aesthetics or functionality.
This technique is especially suitable for patients with minor aesthetic or functional concerns like the so called “ kyphosis” of the dorsum of the nose. ( photos 3-4, 5-6).
Also, certain surgical sequelae of a rhinoplasty can be “camouflaged” with this technique. Some rhinoplasty patients end up with a notorious notch, particularly visible from a side view of their nasal profile. 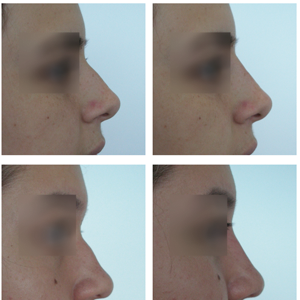
A review of the anatomy of the nose, in particular, the arteries involved in its irrigation is of upmost importance. To ensure safety, the use of blunt tip cannulas is highly recommended 2, 3.
The dorsum of the nose offers the advantage of very loose skin. Because of that fact and considering the softness of Liquidimplant Labium®, the possibility of causing a compartment syndrome-like in this area is remote, in comparison to the tip of the nose, where the skin is tightly bound to deeper planes.
Previous disinfection of the dorsum of the nose with isopropilic alcohol, we apply some anesthetic cream for a period of about 20-30 minutes. I must emphasize that this procedure is almost completely painless!
After removing the anesthetic cream again with isopropilic alcohol, we outline with the help of a surgical pen, the depressed zone to be filled.
Considering the concavities of the areas to be injected, for the comfort of the practitioner, is necessary to bend a little bit the 27 G cannula -some 30 degrees-in order to get the necessary angled direction for entrance in the skin although the cannula is flexible.
We drill little holes for entrance of the cannula using sharp 27 G needles.
And we retroinject along vertical trajects in the outlined depressed zone to be filled. Sometimes it will be necessary to place couple of horizontal injection trajects.
The injection itself must be slowly performed, little by little, with the practitioner standing lateral to the patient, constantly inspecting visually the profile of the nose, in order not to overcorrect. Something remarkable about this anatomic indication is the little volume of Liquidimplant Labium® required: no more than 0.5 ml per average patient. The volume spent, of course, will depend on the severity of the defect to be treated but, in general, this technique requires little volumes of HA.
One of the highlights of this technique and this anatomic indication is the long lasting result: average 2 years before the need of a re-injection!
Besides, in experienced hands, Liquidimplant Cutis® or even Liquidimplant Subcutis ®could be used, with the logical extended duration of the results. But, it is wise to remember that, a learning curve is required to make the move to more viscous presentations of Liquidimplant.
This technique has become more and more requested by patients, because it is safe, effective, long lasting, and even comfortable because of the almost complete lack of pain involved.
1. Braccini F, Dohan Ehrenfest DM. Medical rhinoplasty: rational for atraumatic nasal modelling using botulinum toxin and fillers]. Rev Laryongol Oto Rhinol (Bord). 2008;129(4-5):233-8.
2. Lazzeri D, Agostini T, Figus M, Nardi M, Pantaloni M, Lazzeri S. 2012. Blindness following Cosmetic Injections of the Face. Plastic and Reconstructive Surgery 129(4): 995- 1012.
3. Carle MV, Roe R, Novack R, Boyer DS. 2014. Cosmetic Facial Fillers and Severe Vision Loss. Journal of the American Medical Association Ophthalmology 132(5): 637- 639.
* Omni Hospital Staff Member, Guayaquil, Ecuador
President, Ecuadorean Association of Dermatology and Allied Sciences