Dr Cécile Winter
Rhinoplasty is a common aesthetic procedure but is highly complex. The aim here is to present a reliable and preservative technique, from project to result.
 Anatomical conservative rhinoplasty (ACR) is a preservative type of rhinoplasty. The aim is to keep the amount of tissue damaged by the surgery to a minimum. More than a technique, it is a philosophy: to make rhinoplasty indetectable. How? By keeping certain points of the nose/face balanced and by preserving some of its specific features. There have long been two approaches to rhinoplasty: open rhinoplasty and closed rhinoplasty. Those that prefer the open approach appreciate the fact that they can see the structures properly, whereas those that prefer the closed approach extol the absence of an extended cicatricial area (all of the detached areas) and skin scarring.
Anatomical conservative rhinoplasty (ACR) is a preservative type of rhinoplasty. The aim is to keep the amount of tissue damaged by the surgery to a minimum. More than a technique, it is a philosophy: to make rhinoplasty indetectable. How? By keeping certain points of the nose/face balanced and by preserving some of its specific features. There have long been two approaches to rhinoplasty: open rhinoplasty and closed rhinoplasty. Those that prefer the open approach appreciate the fact that they can see the structures properly, whereas those that prefer the closed approach extol the absence of an extended cicatricial area (all of the detached areas) and skin scarring.
By splitting the nose into two operating zones – the dorsum and the tip – ACR combines the benefits of both the open and closed techniques. This allows the surgeon to visually monitor the osteo-cartilaginous framework while preserving the ligaments between the tip, the dorsum and the skin, for a functional and natural result. This way, ACR is one of the types of preservation rhinoplasty. What is good about this technique is how it can be adapted to different anatomies and its positive predictive value, from the outset of the project to the later results. Here are the key points.
Photo project:
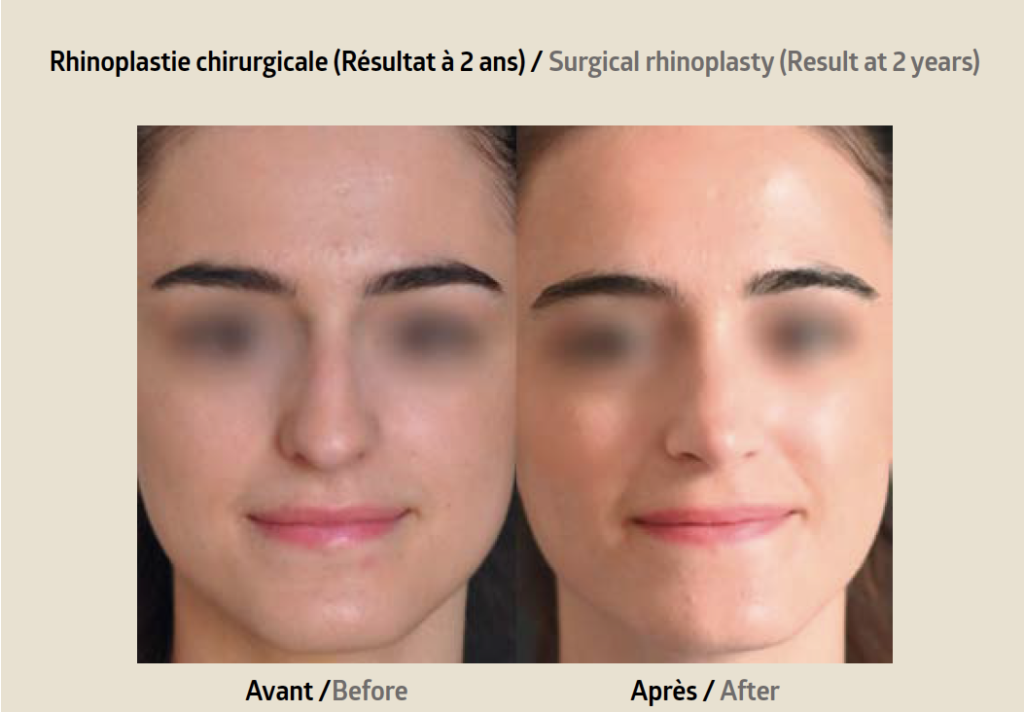
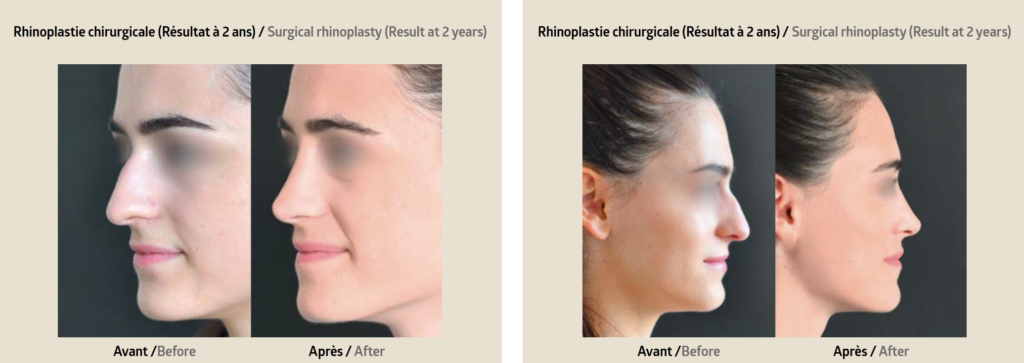
Rhinoplasty is a team effort between the surgeon and the patient. The first question to ask is functional: can they breathe through their nose? Next comes aesthetics: what are the two words that best describe the nose’s flaws, according to the patient? The aim is to highlight the nose’s pre-existing attractive parts; why destroy them with the open approach then rebuild them as they were and risk doing a worse job than Mother Nature? The photos are taken from three angles: profile, head on and three-quarter profile, both static and in movement. This allows us to match the desires of the patient with the technical capabilities of the doctor. To preserve the nose-face harmony, the key point is to preserve the height of the nasal root. This gives the expression its intensity. The tip needs to look realistic. To do this, it is better to adapt the height and length of the dorsum to the real projection of the tip, as opposed to the other way around. The real projection is the top of the soft tissue triangles, not the domes. The tip must remain natural-looking. It can be tilted upwards, refi ned, made more symmetrical, a central fissure might be corrected… The important thing is to ensure its curves remain gentle to keep it looking natural.
The dorsum technique:
For patients, this technique causes no scars on the skin. A first incision is made internally, between the tip and the septum. This allows us to treat the length and height of the septum as well as its straightness and any nasal obstructions. The triangular cartilage (lateral cartilage located below the nasal bone) is detached from the septum and bone, though only in the area the bone is going to be removed.
This way, the bony bump can be removed while preserving the cartilage’s integrity. The bony roof of the nose is then closed up with low, oblique osteotomies, after the mucous membrane has been infiltrated to preserve it and avoid an inversed V shape. To achieve a harmonious dorsum line from the side, face on and three-quarter profile, the triangular cartilage is stitched to the septum to stabilise it using 5.0 stitches. We start by positioning the flaps (autologous grafts to recreate a natural shape with a non-transfixing longitudinal incision). Their folds should correspond to the height of the septum at the top and half a millimetre below towards the tip to properly define the supratip. This way, we achieve a naturally-shaped middle third and we allow for proper breathing over the long term by preserving the internal valve. The now-fixed dorsum can rest while we work on the tip. This leaves the (slightly detached) skin time to adhere to the osteo-cartilaginous framework. This avoids any post-operative irregularities as they will be seen and immediately corrected. The rate of surgical correction is therefore vastly reduced.
Tip:
The incisions are inside and along the lower edge of the alar cartilage (the two pieces of cartilage that form the tip, one right and one left) and stretch from their extremity to the inner edge of the nostrils. The upper side of the cartilage, an area where there are no blood vessels, is detached. This way, the ligaments of the scroll area (which connects the dorsum to the posterior edge of the tip and to the skin), the Pitanguy ligament (which connects the septum to the tip and the skin to the supratip) and the interdomal ligaments (between the right and left cartilage at the tip) are not destroyed. This allows for good perioperative visibility of the result while keeping the skin on the nose’s framework as well as preserving the breathing by maintaining the support at the tip. The cartilage is worked on first, with a minimal posterior cephalic resection in order to define the supratip and the width of the lobule while maintaining the lateral support. Next, trans and interdomal plications are made to achieve nice soft triangles and good definition at the tip.
This way, the inner valve will be preserved so the patient can still breathe properly. The rotation and deprojection of the tip, and the convexity of the lateral crus due to excess length (which could lead to overly-large nostrils) can be treated with a very distal incision of the lateral crus, while preserving the mucous membrane and sliding it upon demand. If the tip is bulbous due to the vertical cartilage at the tip, we may rotate and slide it. This movement is always fixed with a resorbable thread through the mucous membrane. If the tip needs support, it can easily be done by positioning diced cartilage along the nasal spine, which avoids affecting the columella’s structure. We could even insert a columella graft, but this is rarely necessary. A loose, 5.0 stitch between the columella and the septum will stabilise the whole structure and prevent the tip from drooping after surgery. This way, the work done on the tip is mainly preservative, both in the soft tissue and the cartilage, and is stabilised as much as possible, like for the dorsum.
Anatomical preservative rhinoplasty, due to its very limited detachments and the work done separately on the two areas, allows us to see how the light is reflected during the operation, and therefore gives us a realistic view of the nose during the procedure. The preservation of the soft tissue and ligaments preserves the respiratory function and allows the nose to age well. This is a reliable technique that is reassuring for the surgeon and the patients, from the start of the project to the end result.
 Dr Cécile Winter: Anatomist, surgeon and aesthetic doctor of the face and neck, international expert. Passionate about facial anatomy, aesthetics, rhinoplasty and university teaching. In Nice, Pr Castillo and Dr Kestemont have developed the extended marginal approach. Since 2012, thanks to Dr Baris Cakir and his polygon rhinoplasty, I have worked on this double approach. More informations: docteurcecilewinter.com
Dr Cécile Winter: Anatomist, surgeon and aesthetic doctor of the face and neck, international expert. Passionate about facial anatomy, aesthetics, rhinoplasty and university teaching. In Nice, Pr Castillo and Dr Kestemont have developed the extended marginal approach. Since 2012, thanks to Dr Baris Cakir and his polygon rhinoplasty, I have worked on this double approach. More informations: docteurcecilewinter.com