Dr Yuliya Diedyk-Gusarova
Why Amino Acid–Based Tissue Preparation Represents a Biologically Rational First Step in Facial Rejuvenation
Aesthetic medicine has long operated within a volumisation paradigm: identify deficits, fill voids, restore contours. This approach overlooks a fundamental biological variable—the capacity of aged tissue to integrate and retain aesthetic interventions depends on the metabolic competence of the recipient dermal matrix.
The Biological Vulnerability of Aged Tissue

Facial aging reflects progressive ECM failure driven by intrinsic fibroblast senescence and extrinsic environmental insult. Senescent fibroblasts acquire a senescence-associated secretory phenotype (SASP)—upregulating pro-inflammatory cytokines and matrix metalloproteinases—creating a microenvironment hostile to regeneration.(1) UV-mediated extrinsic aging further degrades collagen and elastin, while postmenopausal hormonal decline drives collagen loss at approximately 1–2% annually.(2) In this biologically compromised milieu, variability in filler longevity may reflect differences in ECM integrity and regenerative capacity beyond technical factors alone.
Substrate Availability and Collagen Biosynthetic Efficiency
Collagen biosynthesis depends on adequate intracellular substrate availability. The repeating Gly–X–Y motif of fibrillar collagen requires sufficient glycine, proline and lysine, alongside vitamin C, iron and α-ketoglutarate for post-translational hydroxylation essential to triple-helix stabilisation and cross-link formation.(3) Proline becomes conditionally essential under accelerated turnover; lysine must be supplied exogenously. Impaired hydroxylation reduces cross-link density—a critical determinant of collagen tensile strength. Substrate sufficiency represents a necessary biochemical condition for efficient collagen assembly, though one modifiable component within a broader multifactorial network encompassing fibroblast senescence, oxidative stress and altered intracellular signalling.
Amino Acid Priming: Rationale and Protocol
Amino acid–based tissue priming delivers glycine, proline and lysine intradermally, addressing the structural substrate requirements of collagen biosynthesis. Leucine is included as a metabolic regulator via mTOR pathway activation—supporting anabolic signalling rather than serving as a direct collagen substrate. Non-cross-linked high-molecular-weight hyaluronic acid (HMW-HA) acts as a biophysical conditioner, restoring dermal hydration and viscoelastic properties without structural volumetric expansion. Protocols are delivered as serial intradermal sessions at three to four-week intervals over three to four treatments; structural interventions are deferred approximately two weeks post-completion. Observational data associate this approach with improvements in tissue hydration, elasticity and skin quality—findings that warrant confirmation through randomised controlled trials.
Clinical Integration: Biology Before Structure
The priming paradigm reorders the treatment sequence by addressing metabolic and biosynthetic tissue deficiency prior to structural correction. Patient selection should incorporate assessment of hydration status, elasticity, palpable compliance and systemic variables including hormonal status and medication profile. This framework extends to energy-based and surgical interventions, both dependent on fibroblast viability, ECM organisation and coordinated wound healing. Optimisation of the dermal metabolic milieu may therefore enhance reparative competence across modalities. Amino acid–based tissue preparation represents a biologically rational preparatory strategy whose clinical role warrants rigorous investigation within evidence-based aesthetic medicine.
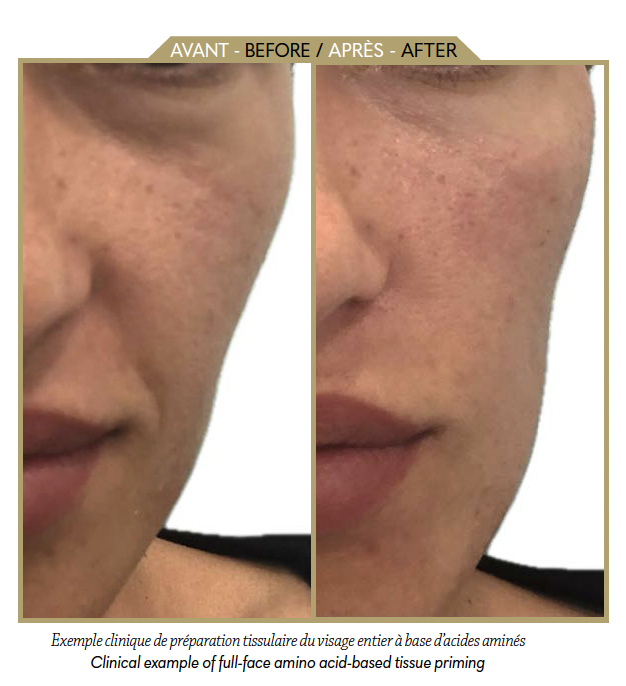
A 41-year-old female patient underwent three sessions of intradermal amino acid-based dermal priming at two-week intervals (glycine, proline, lysine, leucine and non-cross-linked HMW-HA). Clinical photographs demonstrate baseline appearance (left) and three weeks post-completion (right). No additional interventions were performed during the treatment period. Images obtained under consistent lighting and head positioning without digital enhancement.
Dr Yuliya Diedyk-Gusarova

MD — Maxillofacial Surgeon, Aesthetic Physician, and Founder of DrJ Clinic London and DrJ Academy.
Infos: drjclinics.com